
In this month's Body and Embodiment blog installment, Kelly Underman (Drexel University) interviews Amy Chandler about her book Self-Injury, Medicine and Society (Palgrave MacMillan, 2016).
| ASA Section on Body & Embodiment |
|
|
In this month's Body and Embodiment blog installment, Kelly Underman (Drexel University) interviews Amy Chandler about her book Self-Injury, Medicine and Society (Palgrave MacMillan, 2016).
2 Comments
In this month's Body and Embodiment blog installment, Paige Sweet (University of Illinois at Chicago) interviews Dr. Ben Spatz about his book What a Body Can Do (2015, Routledge).
 by Paige Connell and Danielle Antoinette Hidalgo Spoiler Alert: This entry includes information about the end of Season 3 Representations of sex workers on popular shows such as Game of Thrones, The Good Wife, and, of course, any version of CSI, are often stereotypical, completely incorrect, and infuriatingly dehumanizing. Like so many of these shows, House of Cards offers more of the same old sex worker narratives. Yet, House of Cards also offers a somewhat different narrative for a former sex worker and central character, Rachel Posner. The show follows her story for three full seasons, offering some hope that she might enjoy a new narrative that would not end in her death, dehumanization, or any other number of sensational and tumultuous storylines. So, when she is murdered in the final episode of Season 3, any viewer who was paying attention, sensitive to her character’s role as a sex worker, and invested in a new narrative for current and former sex worker characters on popular TV shows, probably felt deeply let down. Her death inspired us to go back and analyze how her role in the series was both intensely invisible and visible. In this short piece, we analyze how Rachel (via her embodied representation) is dehumanized in multiple ways at the same time that her character (from the very first moment she appears on screen) serves as one of the most important characters on the show. She has information and experiences that could reveal murder and corrupt political strategizing orchestrated by the protagonist Frank Underwood. She is the thread that weaves the entire series together. Most characters on the show do not value Rachel beyond worrying about how she could harm them; but the show, too, devalues her. Even the promotional material for Season 1 (pictured above) fails to include an actual photo of Rachel while including images of a number of other characters who were less central to the storyline and appeared in fewer episodes. Yet, whoever arranged the photoshoot didn't think she was important enough to include. Other characters talk about her when she’s not present at all, often referring to her as “the prostitute” or “some hooker,” rather than by her name or anything else that describes who she is or what she does/did in a respectful way. Tellingly, at the beginning of an episode, we watch Rachel making coffee one morning in her small apartment. Yet, instead of watching her, we watch her body parts; the camera pans over her torso, her breasts in a lace bra, and then her legs before we finally see her entire body and face. There is not one single scene even remotely like this for any other character on the show. Another major way that Rachel is marginalized in the context of the show is that she is not given many scenes or storylines that are about her—her private life, time spent with friends, or what’s important to her. This is in contrast to other characters with a similar status. For instance, the audience is made to feel sympathy for Gavin, a hacker, when an FBI agent threatens the life of his beloved guinea pig. In contrast, it is Rachel’s ninth episode before the audience sees her interact with a friend, and we never really learn what motivates her beyond fear and survival. In this sense, Rachel is almost entirely invisible in her own storyline. She only exists when people want something from her. Rachel is also made invisible by the way she is represented or discussed in many scenes. For instance, although she is physically present, she has zero lines in her first couple scenes. After appearing (without lines) in Episodes 1 and 2, Rachel reappears in Episode 7, although she’s not really present; she re-emerges in the form of a handwritten note to Doug Stamper (Underwood’s indispensable assistant). She writes: “I need more money. And not in my mouth.” These are Rachel’s first two lines in the entire series; however, she’s not actually saying them, she’s asking for something, and one of the lines draws attention to a sexualized body part and sexual act that she engaged in with Doug. Without judging the fact that she engaged in a sexual act with a client (granted, a complicated and often extremely coercive relationship with this “client”), what’s notable here is the fact that she isn’t given a voice or her own resources. She is constantly positioned in relation to other characters and without the resources and ability to survive on her own. This can clearly be seen in the way Rachel is easily pushed around by other characters in the show, who are able to force their will upon her. When viewers do finally see her in a friendship, one that blossoms into a romance, the meaning that Rachel gives the relationship is overshadowed by the reaction aforementioned Doug Stamper has to it. Doug has more contact with Rachel than any other character on the show; in the beginning of the series, he acts as a sort of “protector” to Rachel, by finding her a safe place to stay, ensuring that she can work free from sexual harassment in her new job, and getting her an apartment of her own. However, all of these actions highlight the fact that she does not have her own resources or connections to be able to function on her own, and they are used to manipulate her (both physically and emotionally). Over Rachel’s growing objections, Doug is able to impose his wishes upon her fairly easily. The moment she is able to overpower him and escape, she disappears from the show for almost a whole season, only to reappear in the episode where she dies. In this episode, we finally see Rachel standing on her own two feet. It seems like a hard life, working lots of double shifts and living in a rundown boardinghouse, but we also see her enjoying herself with friends and building something new for herself. And yet, it is also in this episode where she has leveraged her competence into a new life that she also meets her demise. Unfortunately, after seeing this vision of Rachel on the road to empowerment, more than half of her scenes relate to her death, and in most of them she is begging Doug for her life, once again reduced to powerlessness. It’s almost as if the show does not have any use for a sex worker (former or otherwise) who can competently manage her own affairs. Perhaps that idea didn’t even occur to the writers because of the place in our society in which sex workers are currently situated, perhaps it disrupts the fallen woman narrative, or perhaps for some unfortunate reason, a death seems more “interesting” than a storyline where a sex worker has agency and takes an active role in shaping her own life and affecting those around her. Whatever the reason, House of Cards ultimately fails Rachel and sex workers, in general. About the Authors  Paige Connell is an undergraduate student at California State University-Chico, currently completing Honors in the Sociology Major. Her main areas of interest include gender, class, and intimate relationships (romantic, family, and friendships). Her honors thesis uses content analysis to look at the depiction of romantic relationships in top music videos with an eye to how they normalize unhealthy and abusive behaviors. She recently completed ethnographic fieldwork for the California Energy Commission that connects tiny houses, technology use, and behavioral change.  Danielle Antoinette Hidalgo is an assistant professor of sociology at California State University-Chico. She completed her Ph.D. (2009) at the University of California-Santa Barbara and her MSc (2001) in Sociology at the London School of Economics and Political Science. Her areas of interest include gender, sexuality, sociology of the body, and globalization. As a graduate student, she coedited Narrating the Storm: Sociological Stories of Hurricane Katrina (Cambridge Scholars Publishing, 2007) and coauthored “The Dyadic Imaginary: Troubling the Perception of Love as Dyadic” (2008). Her work has appeared in Porn Studies, Journal of Bisexuality, Sociological Spectrum, and Journal of Family Issues.
 by Kjerstin Gruys, PhD Assistant Professor of Sociology University of Nevada, Reno A few months ago the website Inc.com featured the essay "Why Women Who Want to Be Leaders Should Dye Their Hair Blonde, According to Science" as it's lead article. As a (blonde) sociologist studying how appearance shapes women's labor market opportunities I read the article with great interest. The research itself seems fascinating and important, but the coverage of it by writer @MindaZetlin is deeply concerning. Zetlin over-extrapolates from the research findings presented by Dr. Jennifer Berdahl and Dr. Natalya Alonso, professors at the University of Columbia's Saunder School of Business, at the Academy of Management's annual meeting. Observing what seemed like an odd overabundance of blonde women in leadership positions, Berdahl and Alonso conducted a study with 100 men, to gauge their reactions to hair color. As summarized by Zetlin, Asked to rate photos of blonde and brunette women on attractiveness, competence, and independence, the men thought all the women were equally attractive, but that the brunettes were more competent and independent. Then they were given photos of blonde and brunette women paired with a quote, such as "My staff knows who's boss" or "I don't want there to be any ambiguity about who's in charge." Suddenly there were big differences, with the brunettes coming in for harsh criticism, while the blondes were rated much higher on warmth and attractiveness. In a Huffington Post interview, Berdahl is quoted as saying "If the package is feminine, disarming, and childlike, you can get away with more assertive, independent, and masculine behavior." In other words, having blonde hair appears to help women more easily navigate the double-bind of being seen as either likable or competent. In my undergraduate Gender & Society course we discuss how overtly feminine appearance work – or “aesthetic labor,” when that work is tied to the labor market – might be understood as a form of “female apologetic,” a gender strategy commonly associated with female athletes who strategically embody traditional femininity as a way to symbolically make up for their participation in stereotypically masculine sports.
I can relate to this. My hair own is naturally blonde, and I've long had a gut sense that I get away with more in terms of non-conforming gender behaviors because of my conforming fair skin and light hair. Looking “girly” (a concept which, of course, is not just about gender presentation but also race, class, sexuality and age), can serve as a social buffer when behaving, well, manly. Berdahl and Alonso's research suggests this gut sense isn’t completely in my (tow)head. I've had (usually female) students come up to me at the end of a course to share that they wouldn't have taken my class – much less feminism – seriously if I hadn’t been "cute" and "fun." I love hearing that my classes are fun and engaging, but I HATE being called "cute." Cute is for puppies, not professors. Indeed, one downside to being "a blonde" is not being taken as seriously. I feel like I have to be consistently articulate and "sound smart" in my professional life to keep colleagues and students from seeing me as I'm dumb or shallow. In fact, during my first semester of graduate school I darkened my hair to brown because I thought I would be taken more seriously. I’m not sure it helped. Maybe it did, but it came at the cost of feeling like myself. These days I instead lighten my hair to a purplish platinum (and I always wear "statement" glasses) because I think it helps me look a little more edgy and LESS "cute." I feel like myself, but it took a lot of overanalyzing to get here. Despite my annoyance with the "dumb blonde" stereotype, having straight blonde hair is a privilege that has helped me navigate many social and professional relationships more fluidly than other women, especially women of color. That said - I abhor Zetlin's suggestion that all ambitious women should lighten their hair. For one thing, the science supporting this contention is incomplete. Berdahl and Alonso's fascinating research has only examined men's perspectives on women's hair color. Given the gender diversity of today's workplaces - as well as evidence that women may make appearance-related attributions differently than men - it is a mistake to believe that only men's perspectives matter. Further, understandings of "good hair" are not merely determined along gender lines, but are matters of race, class, gender, age, and other intersecting privileges. For example, after presenting at an ASA panel on "Embodied Labor & Intersectional Inequalities" last summer, fellow presenter UVA grad student Allister Pilar Plater, and I discussed the observation that some professional Black women maintain chemically “relaxed” hair while climbing the corporate ladder, but transition back to their natural hair texture once reaching positions with greater power. What meanings and consequences come with natural hair for those Black women who choose it, and how are those meanings and consequences shaped by class status? The term “nappy” has often held shameful racist and classist connotations, but today the term has been reclaimed and embraced by some black women, from bell hooks who wrote the children’s book Happy to Be Nappy to the trending hashtag #NappyAndHappy. But can poor Black women claim #nappyandhappy in the same way as more privileged Black women? More intersectional research is needed before we can make confident claims about the multiple meanings and consequences of women's hair strategies (much less give proscriptive advice on what women should do). The decision to "go blonde" or chemically “relax” hair incurs real risk alongside any potential upside. The expense, time commitment, and unknown risks of chemical exposure involved in high-maintenance hair color and/or texture might very well outweigh the social benefits any individual woman might hope to enjoy. Time, money and health are not minor sacrifices. The upkeep of my own purplish platinum hair, for example, demands 2-3 hours of idle time every 6 weeks and costs more than my monthly gym membership. I justify it as an aspect of my "don't call me cute!" personal style, because time in the salon feels like self-care, and because it turns out that extremely damaged hair doesn't have to be washed as often as my natural hair texture (so I can make up for some of that time lost in the hair salon). I also believe – perhaps idealistically – that having purple-toned platinum hair is an expression of diversity rather than conformity (at least in the academy!), and that my visible non-conformity might have little consequence for me, while helping to make space for others. These are the things I consider in my most innocent personal calculations, but, of course, it is ultimately my class and race privilege that allow me to indulge in the considerable expense of "having fun with my hair" and "playing with color," while less privileged women – especially those whose natural hair color and texture are the opposite of mine – can neither afford such indulgences, nor are likely to find them quite so "fun" if they are pushed by the pressures of discrimination rather than pulled by the pleasures of aesthetic experimentation. And here is where Zetlin is so wrong to say that, "women who want to be leaders should dye their hair blonde." Sure, there may be some sound personal "strategy" in doing so (alongside, of course, the risks), but viewing appearance discrimination as an individual problem that individual women should solve by changing their bodies is dangerously short-sighted. It's just one more "patriarchal bargain" that privileges some women (usually those already privileged) while perpetuating a fundamentally unequal system. ... Author Bio: Kjerstin Gruys is an Assistant Professor of Sociology at University of Nevada, Reno and author of Mirror, Mirror, OFF the Wall: How I Learned to Love My Body By Not Looking at It for a Year (Avery, 2013).Kjerstin's research broadly explores the relationship between physical appearance and social inequality, with a particular focus on gender as it intersects with race/ethnicity, class, sexuality, and age. She has specific expertise in: (1) Labor Market Inequality & "Aesthetic Labor," (2) Intersections between Bodies/Embodiment and Cultural Markets, and (3) How News Reporting on Obesity & Eating Disorders Shapes Prejudice and Health Behaviors. Her research - empirically grounded through ethnography, in-depth interviews, content analysis, and the occasional experiment - has been published in Social Problems and Social Science & Medicine, among others. Prior to earning her PhD from UCLA (2014), Kjerstin worked as a merchandiser in the corporate offices of two multi-national fashion firms. She is currently developing a book manuscript, tentatively titled: True to Size?: A Social History of Clothing Size Standards in the U.S. Fashion Industry.  by Randolph Hohle, PhD
Assistant Professor of Sociology Fredonia, SUNY Critics, pundits, bloggers, and just about everyone with a pulse and a social media account have taken to the public sphere to explain how Hillary Clinton, the most unpopular candidate ever to win the popular vote, lost the presidential election to Donald Trump, the most unpopular person ever to occupy the executive branch. Blame was evenly distributed but didn't explain much. Although data indicated that the medium income of the Trump voter was $72,000, it was the fault of the white working class. It was also the fault of anyone without a college education as well as rural whites. Rural whites make up a paltry 17% of the entire electorate. Rural whites haven't supported a Democratic candidate since the south was a one party system and Franklin Roosevelt was president. It was white women’s fault because more white women voted for Trump than Hillary. However, more white women voted for Mitt Romney over Barak Obama four years ago, just as more white women voted for John McCain over Obama in 2008, which means that white women simply voted like white women have in recent elections when the Democrat’s candidate won. It was the fault of blacks because blacks cast fewer ballots in 2016 than in the previous two elections. Republicans managed to suppress minority voters with racist Voter ID Laws and other implicit racist tactics, such as supplying limited voting machines in minority precincts. Only stalwart leftist magazines like the New Republic pointed out that Trump's support was found in the upper and middle class white suburbs, comprised of the very people who thrived after the recession, and were not affected by the last few decades of deindustrialization. On the positive side, it may have been the first time no one blamed black women for an undesirable outcome. I'm not here to add to the cacophony of the blame game of why Hillary lost. It's not very productive. I am here to advocate for the importance of the body as an independent variable. Bodies have agency in the sense that bodies exert an affect over political outcomes. I've done so elsewhere. I've explained how exercising power over one's body can produce changes in others and how the performativity of protests can fuse protesters with audiences. I've explained how the tension between racially threatening and racially non-threatening bodies continue to hinder struggles for racial equality and how good white bodies are an integral part of the neoliberal project. Others have as well. Marion Klawiter explained how different fields of contention formed around the bodies of breast cancer survivors and breast cancer victims. The events leading up to the 2016 election and waves of post-election protests provide an opportunity think how a network of white bodies formed a racist white public in relation a profaned meta-public comprised of brown bodies, sick bodies, trans bodies, migrant bodies, and the bodies of refugees. Publics and public spheres have to be created. They do not simply exist, waiting around for us to enter. Judith Butler's recent entry into the debates around performativity and assemblages explains the relationship between bodies and the making of publics. As Butler explained, bodies still come together with the streets to form a public, "No one body establishes the space of appearance, but this action, this performative exercise happens only between bodies, in a space that constitutes the gap between my own body and another’s. In this way, my body does not act alone, when it acts politically. Indeed, the action emerged from the between.” Publics are the means for marginalized groups to get their demands for equality into the broader political agenda. Publics make invisible groups and invisible bodies visible. In turn, Butler notes that the process of making a public "contests the distinction between public and private." Butler, always the eternal optimist, imagines how an assemblage of a public can grant marginalized bodies a political voice. I'm not so optimistic. Marginalized groups have a limited control over how audiences respond to their claims. In the neoliberal era, the visibility of marginalized bodies triggers a white backlash -- especially when racialized and other threatening bodies are visible. Political audiences and political parties have been segregated since the end of the civil rights movement. In the early 1970s Richard Nixon foresaw the existence of the Voting Rights Act as a political marker that would drive disaffected white voters to the Republican Party. Lyndon Johnson was the last Democratic president to win the majority of the white vote. Real instances of racial integration and the existence of pro-civil rights legislation trigger a white response. Each white response is an additional wave of neoliberal reform. Republican's rallied white voters against the 1993 Motor Voter Act via the myth of fraudulent black voter. Along with strategic gerrymandering, Republicans took control of congress in 1994, setting the stage for banking and pharmaceutical deregulations, and the privatization of social welfare. Obama's presidency set the stage for another potential wave of privatization, austerity, and more tax cuts for the wealthy. The key site of political struggle in the contemporary public and public sphere has increasingly shifted from a discursive struggle to a corporeal one. The body appears prior to a movement's claims for equal citizenship. The body is a form of communication at the visual and affective level that simplifies complex political and economic policy into simple ideological categories of liberal and conservative. The body communicates political meanings, narratives, and myths, and in turn, connects audiences with distinct publics. Audiences read publics as sympathetic, dangerous, or subversive; as sacred or profane; as good or bad. In the current digital age of rapid news feeds made up of staged photo-ops, selfies, memes, gifs, scrolls, likes, and swipes -- talk is downplayed. The importance of corporeal politics has increased in the digital age. The question is not just how embodied performances create publics. But rather, how elites and ordinary citizens bind and fail to bind heterogeneous publics together. The binding of heterogeneous publics illustrates the assemblage of a meta-public. A meta-public is not simply comprised of a network of specific publics. It also captures an outcome, a dependent variable if you'll have it, which is the current political climate. To give a contemporary example of how bodies lead to the assemblage of a meta-public in the US, let's consider the elite and middle class white response to the increased visibility of brown bodies since Obama's second term. I define brown bodies as Arab bodies, black bodies, latino/a bodies, and Muslims bodies. In every case, the brown body serves as the focal point to influence the audience response to the public. Depending on the audience, a public of black bodies protesting police brutality can be a demand for reform or a riot. As the collection of local anti-racism and anti-police brutality groups assembled under the tag line #Blacklivesmatter, whites responded with their own tag line: #Bluelivesmatter. #Bluelivesmatter was not just a defense of the police. It was an affirmation of white supremacy, of racial discrimination, of legitimating the state violence against marginalized brown bodies. The brown body provided a figurative focal point for middle class whites' to link their own domestic anxieties with global and economic changes. The brown body is always nomadic -- a stateless actor -- that threatens white borders and steals white jobs. The visibility of Arab and Muslim bodies define the terrorist public that threatens whites' sense of security. White Christian terrorists, white men and their guns and homemade bombs, are responsible for the overwhelming number of domestic terrorist acts. Yet, whites do not demand deporting other whites, they do not criminalize Christianity, and they do not place restrictions on easy gun access. The visibility of latino/a bodies connects legal and illegal immigration with global economic insecurity. Deindustrialization, driven by a combination of increased use of robots and automation in manufacturing, federal tax policies that supported relocation of firms from the northeast and great lakes region to right to work states in the south, the recent popularity disruptive business practices, and the privatization of social welfare since the 1980s, has eroded the value of real wages in the United States. It was not Mexican immigrants. But bodies carry mythologies that are more potent than data driven facts when influencing political ideology. Brown bodies create different publics than trans bodies. Trans bodies subvert and undermine the gendered world order. The bathroom is reconstituted as a public as trans bodies come together to demand open access and equal use of a facility designed simply to relocate bodily wastes to a sewer treatment facility. The social conservative response to visibility of trans bodies was to assemble a new anti-gender equality public dominated by the bodies of heteronormative white men. The new anti-gender equality public linked with other publics: anti-black, anti-immigration, and anti-Arab. It was the affirmation of patriarchy via men's ownership of women's bodies. When pro-trans activists hold signs that read "It was never about bathrooms" I have a feeling the social conservatives concur. Does the process of assembling a meta-public exist on the left? Clinton jammed the various racist, neo-nazi, sexist, and homophobic publics into a single alt-right public, or basket of deplorables. But the left has been unsuccessful in linking the alt-right with neoliberalism, which in my humble opinion must be done. This may indicate how the left's inability to think of an alternative political and economic project to neoliberalism leaves them unable to create links with other publics. Or it may indicate that elite whites in the Democratic Party who've benefited from neoliberalism over the years aren't as liberal and progressive as they think they are. It's an empirical question. In short, publics don't just exist, but once they are created and a link is forged between publics, a pathway is created for the actor to take a stroll through the various publics. The stroll may be voyeuristic. It may be life affirming. But the connections that are made and not made involved eyes interpreting bodies. Not all is bad. In urban areas where whites tend to be more liberal, they are willing to create coalition districts with minority groups and vote for minority candidates. However, states with a large minority population and a republican governor were also more likely to pass laws to limit minority votes, such as Voter ID laws. In any case, I hope my brief blog post highlighted one way that the body as an independent variable can be used to study politics. I think body and embodiment scholars have still only begun to scratch the surface on the potential contributions that an embodied perspective adds to our understanding of social movements, collective behavior, and political sociology.
This week, UIC Postdoctoral Research Fellow Kelly Underman talks to Kristen Barber, PhD, about her new book, Styling Masculinity: Gender, Class, and Inequality in the Men's Grooming Industry (Rutgers University Press, 2016). Q1. Congratulations on your new book! Perhaps the central tension you explore is the notion of the “beautiful man”: beautifying body projects and masculinity seem fundamentally at odds with one another. And yet, as you demonstrate clearly in your book, men use beautifying body projects to establish their positions in hierarchies of race, class, sexuality, and gender. What drew you to researching this topic? Were you surprised by your findings? Kristen Barber: When I first started asking questions about gender and beauty, I was interested in women. I don’t think it’s a coincidence that as a woman I take beauty and bodies seriously as sites of scholarly investigation. This is very much related to feminist assertions that researchers’ biographies shape the questions they ask. And since women have been historically dubbed gendered bodies before rational beings, the cultivation of embodiment is a clear avenue for understanding the operations of gendered power. But there is already a proliferation of great work on the racialized and classed politics of women’s beauty regimes, and so I quickly realized men’s aesthetic-enhancing practices was an empirical gap that needed filling. Much masculinities scholarship focuses on men in what we might consider to be predictable sites and practices: body-building, blue-collar work, fathering, etc. I wanted to know more about what it takes for men to negotiate and successfully cross gender-boundaries that might compromise their access to heteromasculine entitlements. What I found was that these men don’t actually risk much at all. Instead, the white men who spend money to have their hair styled, their nails buffed, or their backs waxed at the men’s salons in my study do so as a reflection of their race and class privilege. And these salons are organized in ways that provide clients the resources to in-turn project, at least momentarily, culturally rewarded masculine identities. They can drink imported beer while they wait for their haircut, for example. They can thumb through a copy of Golf Magazine and watch the news while their heads hang in shampoo bowls. But most important in helping these men feel like class-privileged straight men--while they enjoy a complimentary scalp massage--is the expansive labor performed by women salon employees. Q2. In your book, you outline several fascinating examples of how cultural artifacts are remade in order to sell beauty to economically-advantaged men. For example, you mention that “hair dye” is called “color camo” and a manicure is a MANicure. There’s been some attention recently on social media to #masculinitysofragile and the gendered marketing of beauty products to men. In what ways does selling manly beauty products demonstrate the fragility of masculinity, and in what ways does it demonstrate the dominance of masculinity? Kristen Barber: The men’s grooming industry sells men beauty by not calling it beauty. This is evidence that masculinity requires ongoing collective efforts; that it is a fragile concept rather than a biological trait. At any given time, men’s associations with idealized masculinity may be called into question, and so there are cultural rules for men to follow if they want to avoid feeling, or having friends and family accuse them of being, effeminate or gay. And rule number one is still: repudiate the “feminine.” “Beauty” is a feminized term associated with vanity, and if a Cartesian mind-body dualism continues to shape our understanding of who men are supposed to be (rational minds, not emotional or decorative bodies), then they can’t legitimately participate in beauty or be “beautiful.” It is conceptually impossible. This is why the owner of The Executive refers to her salon as a “men’s grooming environment.” This phrase is stamped across the glass front door of the salon. And the women working at The Executive told me that they aren’t supposed to use the term, “salon.” After all, women go to salons. Salons are popularly presumed to be places of vanity and gossip. Men go to barbershops. So, how do Adonis and The Executive sell men a third place that provides the pampering experience of the “women’s” salon but the masculinizing experience of the barbershop? The spaces, products, services, and practices are re-coded both linguistically and symbolically. The salons’ clients pick up on these distinguishing efforts and use the new rhetoric to frame their understandings of the salons; so that they might convince themselves and others that what they do at Adonis or The Executive is unlike what their wives do. One client explained he became a loyal client when he realized that “women’s” hair dye is not “pH-balanced” for a man. Instead, the “hair camo” stylists use at The Executive is made for men. And so he belongs at The Executive; he has to go there to get the appropriate product. Popular notions of biological maleness become key strategies for re-coding beauty practices and products as “for men.” Men can become men when they go to a “grooming environment” to camouflage their grey hairs. This rejection of femininity reveals the value we give to masculinity and the everyday rewards and structural power that come with men’s accomplishments of a certain masculinity. Q3. One of the aspects of your analysis that I found most fascinating is your focus on the labor performed by the mostly women salon employees at your two field sites. You argue that these employees engage in heterosexual aesthetic labor to in order to sell beauty products and services to men. In addition to the emotional labor required of intimate service work, women also socialize men on how to use these products and services, while also themselves performing an embodied form of heterosexual femininity to reassure their clients that beauty is for straight men. In what ways do these insights challenge existing scholarship on embodied emotional labor? Is this a phenomenon particular to these kinds of upper middle class white men’s spaces, or are there other examples? How does this expanded theorizing of labor in service work help scholars to make sense of late modern consumerism and its attendant body projects? Kristen Barber: Styling Masculinity contributes to the scholarship on embodied emotional labor by moving beyond the smile. Providing good customer service in the beauty industry requires ongoing, intimate contact. Hairstylists massage men’s scalps and ruffle their fingers through men’s hair. Nail technicians rub men’s hands and calves. Bodies collide in unique ways in the grooming industry. It is therefore an excellent site for studying emotions and bodies in both service work and consumption. My work focuses on the ways this intimacy is sold as pampering but organizationally interpreted as potentially emasculating for men. In this case, bodily labor actually begets emotional labor and so I theorize “the labor of consumption” in a way that reveals the symbiotic relationship between emotions and touch. For example, women beauty providers told me that they have to mitigate men’s unfamiliarity and discomfort with pampering to assure them they are still men when they get a facial. And when women rip the hair from men’s backs, they assure clients that they are no less masculine for feeling and expressing pain. The women do masculinizing emotional labor because of the gendered meaning of particular touch in a particular space. Yet men working at these salons operate by what I refer to as different “touching rules.” They touch less and touch their clients in different ways--avoiding the facial, shortening the scalp massage, and welcoming their clients with a high-five rather than a hug and kiss on the cheek. I discuss the importance these touching rules play in relieving men of commodified bodily labor and the extra emotional labor required from women. This sort of bodily and emotional labor is specific to white middle and upper-middle class places that emphasize leisure and luxury. But it would be interesting to see how these processes play out in the gay spaces of West Hollywood or in salons that attract more men of color. I would expect sexuality and race to intersect with gender and class in different ways, so as to mollify the social injuries these men experience. Expanding theories on labor as embodied reminds us of sociologist Carol Wolkowitz’s warning not to think that in a deindustrializing society we use our hands any less. In service work, hands are still the tools of production and so scholars should center bodies in their theorization of labor. By theorizing “touching rules” and masculinizing emotional labor as part of larger “heterofeminine care work,” my work emphasizes the fully embodied work that goes into creating the consumer, and by extension the worker. Q4. You detail the challenges of “studying up” as a woman looking at men’s beautifying body projects. What advice do you have for other scholars on how to research men’s body projects? Gender certainly impacted your rapport with the men who frequented your field sites, but what aspects of race, class, and sexuality also shaped your research? Did conducting the research influence your own beautifying body projects in any way, either to help you gather the data or otherwise? Kristen Barber: Every time I teach Qualitative Methodology, graduate students dig into debates about who can study whom, under what circumstances, and whether it’s better for researchers to study people “like them.” Indeed, there is something to be said for more easily accessing and building rapport with participants who might assume you both see the world in the same way. Being a woman helped and hindered me in interviews with women beauty providers. They were open with me about their unflattering opinions of their clients, and I doubt they would tell a male researcher that men are suckers for buying product and “think” more with their penises than with their brains. On the other hand, they often proclaimed: “You know men!” This assumed shared understanding of men made it difficult at times for me to get detailed descriptions of how workers felt about their clients. But I am absolutely sure that being cisgender, straight, associated with an elite-private university, and white helped me to fit in at these high-service salons. My own embodiment, or habitus, helped me to blend in. I belonged. However, as a woman who doesn’t spend a lot of time, money, or effort on cultivating a careful aesthetic, I did worry I wasn’t quite hip enough to spend time in these salons. I found myself paying a lot of attention to my hair and clothes and relating to my body in new ways. I suppose you could say I became more acutely aware of my cisgender appearance, as well as of how this appearance allows me access to well protected sites and privileged people. I believe it is important for researchers to be aware of these things to better understand how they are never not embodied, and how their social status and relationship to power affects their data. Q5. In what ways does your work help us as scholars of the body and embodiment think about the body as both a surface for expressing status differences and as a vehicle for experiencing the world through privilege and inequality? Kristen Barber: In Styling Masculinity I emphasize the ways organizations discipline bodies, but in ways that create both powerful consumers and opportunities for commodified workers to find job satisfaction. The creation of bodies and identities is enabled and constrained within organizations drawing from and reimagining popular tropes of masculinity and femininity. Adonis and The Executive do not just shore-up men’s bodies but allow for particular masculine and feminine bodies to be simultaneously created, so that women become embodied sites of tertiary consumption at the same time men engage class-privileged, exclusionary practices. This simultaneity is a core focus in my book for understanding the dynamic relationship between embodied privileges and inequality. You can find out more about Styling Masculinity and purchase a copy at Rutgers University Press.  Kristen Barber is Assistant Professor of Sociology and faculty affiliate in Women, Gender, and Sexuality Studies at Southern Illinois University, Carbondale. Her book, Styling Masculinity: Gender, Class, and Inequality in the Men’s Grooming Industry, was recently released by Rutgers University Press and has been highlighted in The New York Times, Playboy, and NPR’s Marketplace.
 by Kelly Underman, PhD Postdoctoral Research Associate Department of Medical Education University of Illinois at Chicago In classic studies of socialization in medical school, scholars wrote of the anatomy lab as a foundational experience for the formation of the physician-in-the-making’s self (see Becker, et al, 1961; Fox, 1988; Smith and Kleinman, 1988; Hafferty, 1991). By working with dead bodies during cadaver dissection, the medical student learned how to hide feelings of anxiety, disgust, and sadness. These formative experiences prepared future physicians for working with patients as passive objects under the medical gaze. 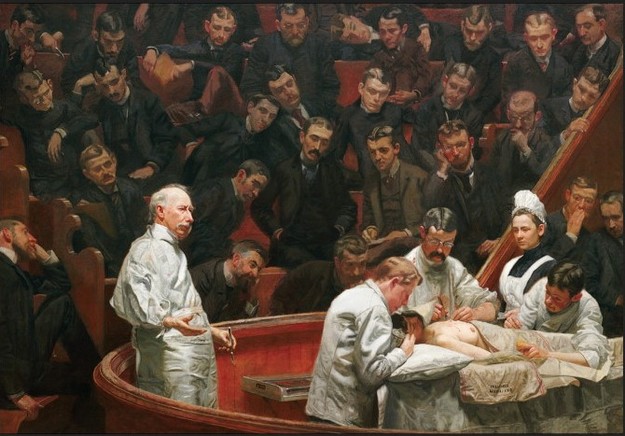 Thomas Eakins, The Agnew Clinic (1889), Source: Atlas of Science And yet, there has been a massive transformation in medical education in the past two to three decades. A range of simulation technologies now add to or fully substitute for cadaver dissection. Medical students work with simulated or standardized patients (real people who roleplay as patients for the purposes of teaching and evaluation), haptic simulators (plastic models with pressure-plates that feed information to a computer), virtual reality technology, and so forth. Furthermore, gone is the old model of physician authority that demands passive patient-objects. Patients are to be engaged with, and empathy is to be valued, not suppressed (Underman and Hirshfield, 2016). In fact, in order to be a licensed physician in the United States today, medical students have to pass an exam that tests their ability to effectively and empathetically communicate with patients. During this exam (called “Step 2”), medical students interact with standardized patients who pretend to have an illness or injury, and the medical student’s performance is graded by both the standardized patients and a board of medical experts.  Students observe an interview with a simulated patient, Source: C3NY.org Simply put, the world of medical education has changed. The kinds of bodies medical students interact with as part of their training are more varied than ever, and the meanings attached to these bodies are radically different. And yet, few scholars have considered what this means for theories of socialization in medical school. How might new theories of the body and embodiment help explain contemporary medical education? Critiques of (bio)medicine in the past three decades have advanced the idea that the patient’s body is socially constructed. Drawing on path-breaking works such as Michel Foucault’s Birth of the Clinic, scholars have demonstrated that the patient-body is produced as an object under the medical gaze through a range of techniques, practices, and discourses. As such, critics of biomedicine have unpacked how the patient-body is constructed in a myriad of contexts. In more applied contexts, scholars in the health humanities and health professions education have attempted to re-instill notions of the patient as more than just a body-object into medical trainees. However, while the construction of the patient-body has been thoroughly interrogated, few scholars have considered the construction of the physician-body in biomedicine. I consider this very question through the lens of the medical habitus (Underman, 2015). The medical habitus “allows scholars to move beyond purely cognitive models of socialization to consider the transformation of thoughts, perceptions, feelings, and embodiment of medical students as they adapt to medical culture” (Underman, 2015: 181). Previously, scholars of socialization in medical education examined how the medical student learns to play “his” role in the clinic, as in Howard Becker et al’s classic study Boys in White. Other scholars, such as Frederic Hafferty, described the role of the hidden curriculum in medical student socialization, demonstrating how latent rules and norms transmit lessons about medical values. While these perspectives are important, I argue that using the medical habitus as a framework to understand the adoption of a professional (clinical) identity better captures the embodied and emotional (or affective) dimensions of this medical socialization. My research examines how medical students learn the pelvic exam on a specially-trained layperson called a gynecological teaching associate (GTA) I selected GTA programs as a case study to understand how simulated patient experiences lead to the adoption of the medical habitus. I show in my work that GTA programs emerged in the 1970s and 1980s in response to critiques in the Women’s Health Movement about how medical students were taught the pelvic exam—usually on indigent clinic patients. Around the same time, medical educators were launching similar critiques of how the pelvic exam was taught. These educators argued that existing models were ineffective because students were often too nervous or unable to ask questions of either their faculty or the person they were examining. GTA programs addressed these critiques by using trained laypeople to teach the pelvic exam. In a typical session, a GTA will walk a group of two to three medical students through a complete, patient-friendly pelvic exam using the GTA’s own body as the model (Underman, 2011). These programs have become ubiquitous, with over 90% of medical schools in the United States and Canada using GTAs (Beckmann, et al, 1988).  Students work with a gynecological teaching associate, Source: The Washington Post GTAs are one type of simulated patient encounter that today’s medical students experience. As I show in my work, the use of simulation allows medical students to practice and develop their clinical skills, dispositions, and attitudes in a low-risk environment. Because GTAs are not ‘real’ patients, they allow medical students to explore the performance of a pelvic exam in a much more in-depth fashion, while at the same time offering feedback and instructing the students about anatomy. The GTA session is particularly interesting to study because the pelvic exam is so emotionally-fraught. Medical students are often extremely nervous about hurting the patient or embarrassing themselves (or the patient). Not only that, but reproductive anatomy and female bodies evoke uncomfortable associations with sexuality that medical students must learn to manage if they will successfully become ‘professional’ physicians. The framework of the medical habitus is useful here because it allows me to focus on the range of embodied dispositions and attitudes that medical students adopt during the GTA session, especially with regard to emotion. Norms and values about centering the patient in the pelvic exam and involving the patient actively in their own healthcare become embodied in complicated and sometimes contradictory ways. This is especially important, as there has been a shift recently toward an increased emphasis on empathy in the clinical encounter (Underman and Hirshfield, 2016). In the GTA session in particular, empathy is as much an affective state as it is a performance of skills and behaviors necessary for eliciting the patient’s cooperation. For example, during the speculum exam, medical students are taught strategies like using non-threatening language (“bills” instead of “blades”) and giving the patient a warning touch on the inner thigh before making contact with the genitals. These strategies ostensibly are for the patient’s comfort and relaxation. However, they also make the physician’s job of performing the exam easier, since a relaxed patient is more compliant. The crafting of the physician-body in medical education is a fascinating topic and ought to be considered by more scholars studying the body and embodiment. Scholars in science and technology studies (Prentice, 2012; Harris, 2016) have considered this more in-depth, and it remains an important topic for consideration. Through my work, I argue that we should consider how it is that patient-bodies and physician-bodies are constructed through an entanglement of discourses, practices, and techniques in medical education. We know that bodies don’t exist in isolation of the social practices and structures within which they move, and medical school is no exception. By exploring new technologies of simulation and drawing from new theoretical tools, I intend to more fully understand what happens to the medical gaze when the patient sits up and talks back. ---- Kelly Underman, PhD, is a Postdoctoral Research Associate in the Department of Medical Education at the University of Illinois at Chicago. Her research interests include medical education, the body and embodiment, affect studies, and the politics of knowledge production. Her work has been published in Social Science & Medicine, Gender & Society, Social Studies of Science, and Sociology Compass. Citations
Becker, Howard S., Blanche, Geer, Everett, C. Hughes, Anselm, L. Strauss, 1961. Boys in White: Student Culture in Medical School. University of Chicago Press: Chicago. Beckmann, Charles R. B., B. M. Barzansky, B. F. Sharf, and K. Meyers. 1988. “Teaching Gynaecological Teaching Associates.” Medical Education, 22 (2): 124-31. Fox, Renee C., 1988. Essays in Medical Sociology: Journeys into the Field. Transaction Books: New Brunswick, NJ. Hafferty, Frederic W., 1991. Into the Valley: Death and the Socialization of Medical Students. Yale University Press: New Haven. Harris, Anna. 2016. "Listening-touch, Affect and the Crafting of Medical Bodies through Percussion." Body & Society, 22(1): 31-61. Prentice, Rachel. 2012. Bodies in Formation: An Ethnography of Anatomy and Surgery Education. Duke University Press: Durham, NC. Smith, Allen C., Kleinman, Sherryl, 1989. “Managing Emotions in Medical School: Students’ Contacts with the Living and the Dead.” Social Psychology Quarterly, 52(1), 56-69. Underman, Kelly. 2011. “’It's the Knowledge that Puts You in Control’: The Embodied Labor of Gynecological Educators.” Gender & Society, 25(4), 431-450. Underman, Kelly, 2015. “Playing Doctor: Simulation in Medical School as Affective Practice.” Social Science & Medicine, 136-137: 180-188. Underman, Kelly, and Laura E. Hirshfield. 2016. "Detached Concern?: Emotional Socialization in Twenty-First Century Medical Education." Social Science & Medicine, 160: 94-101.  by Dana Berkowitz, PhD
Associate Professor of Sociology and Women's & Gender Studies, Louisiana State University The perfect combination of prom queen-pretty with sophisticated conservatism, Dawn Goldstein is 5’9”, has big blue eyes and a perfectly coiffed blonde mane. As a former beauty queen, Dawn Goldstein was socialized early on to learn that her social currency largely derived from her ability to achieve and maintain a youthful, beautiful face and body. From a very young age, Dawn was taught how to cultivate her appearances through exercise, dieting, make-up, and other kinds of bodywork in order to look young, healthy, and pretty. When Dawn was twelve years old, she was sent to a plastic surgeon by her father to have her ears pinned back. When she was fifteen she learned to count calories. When she was twenty-eight, she had laser hair removal on her bikini area, legs, and underarms. And when she was thirty-three, she began using Botox. I met Dawn in 2012 when I was collecting research for my book, Botox Nation: Changing the Face of America (NYU Press). On the surface, Dawn Goldstein fulfilled every societal stereotype of a woman who would use Botox in her 30s. She was a former beauty queen, she was always impeccably groomed, and she was thin, tall, and attractive. However, my three-hour conversation with Dawn proved that such one-dimensional assessments and stereotypes miss some critical insights about women who use Botox, obscuring the complexities of women’s social psychological decision making about their aesthetic labor. Dawn, a self-identified feminist, spoke at length about the tensions permeating her decision to use Botox and about her frustrations with the ubiquitous cultural pressure to accommodate to societal norms of feminine attractiveness. As a former beauty queen, Dawn always had to be very conscious of her face and her body. Now, as an adult and a successful broadcast journalist, she was even more aware of the cultural pressure she faced to preserve her youth and beauty. Ultimately when she turned 33 and found that her monthly facials and expensive creams would no longer suffice, she resigned herself to trying Botox. Dawn was adamant that if she were not on television each day, if her career hadn’t depended on it, she would have likely made a different decision about using Botox in her thirties. Eventually, her desire to stay on television superseded both her feminist ethics and any desire to age without technological intervention. Dawn’s experience mirrors that of so many other Botox users with whom I spoke. Like others, she engaged in a lifetime of bodywork, a sociological concept that refers to the efforts people exert on their own bodies to attain certain bodily ideals through diet, exercise, makeup, clothing choices, and cosmetic surgery in the hopes of achieving high social status (Gimlin 2002). Yet, that Dawn explicitly turned to Botox because of workplace concerns reveals the need for sociologists to consider how regular forms of body upkeep are distinct from those forms of bodywork used to present the body as a legitimate workplace commodity. Many of the women with whom I spoke articulated their decision to use Botox as a means for improving the enterprising self and as a practical and necessary upgrade to maintain their competitive edge in the workplace. Women in the service economy were especially likely to mention the importance of engaging in aesthetic labor for their careers. Katherine Turner, a manager at a Miami high-end boutique told me, “Appearances are central to this job. My face is like my business card. There is no way I can afford to look tired or old.” Sociologists Christine Williams and Catherine Connell (2010) have argued that the workers employed at upscale retail stores are a large component of what is purchased; they literally embody the intended cultural meanings associated with the products and services sold in the shop. In this way, the commodification of workers’ corporeality naturalizes those embodied distinctions that are shaped by social inequality. As Dawn Goldstein’s story foreshadowed, the theme that Botox injections were a career investment was particularly evident among the broadcast journalists in my sample. Allison Harris, a broadcast journalist in Louisiana, shared that, “With my situation a lot of it does have to do with the job. I mean I want to be able to stay in this business for a while; I’m not independently wealthy. I need a job. And the longer I can preserve my appearance and as much youth as I can, the longer I’m going to be able to stay in the business for years and years and years.” In order to succeed in their workplace, women felt they needed to look better, fresher, and more confident. As body entrepreneurs who strategically cultivate their appearances in order to enhance their social, cultural, and economic power, Botox users emphasize the legitimate desire for career advancement and workplace prosperity. Reflective of American values of industriousness and hard labor, these women spoke about investing in their bodies to sustain their competitive edge in commercial economies. Couching their explanations of aesthetic labor within masculine tropes of competition, they fashioned themselves as ambitious and motivated careerists. Where on one end, aligning femininity with such brazen determination contrasts from stereotypical constructions of traditional middle-class femininity as docile and passive; however, that their source of power came from their beauty and bodies revealed how women’s entrée into male dominated occupations has not corresponded with the freedom to abandon the pursuit of the feminine beauty ideal. My interviews with Botox users can tell us a great deal about the transmission of social inequality through bodies. Because bodies are read as signs of success, they can be used to access other avenues of success. Through deliberate cultivation of their embodied cultural capital, individuals can also accumulate economic capital. Yet, it is important to keep in mind that regular Botox injections are out of reach for much of the population. Most women do not have basic healthcare, let alone the disposable income to purchase Botox – a procedure that averages approximately $300–$400 for one round of injections. Oh, and did I mention that Botox is only temporary? So if you want any lasting effect, you are supposed to top it off two to three times a year. Most American women cannot afford anything close to what such a regimen requires. Thus, my research on Botox users reveals how some body modification practices can increase gendered social stratification by exacerbating existing economic inequalities. ----------- Dana Berkowitz, Ph.D., is an Associate Professor of Sociology and Women’s and Gender Studies at Louisiana State University. She received her Ph.D. in Sociology with a certificate in Women’s and Gender Studies from the University of Florida in 2007. She is the author of Botox Nation: Changing the Face of America (NYU Press). Her scholarship has also appeared in high-impact journals such as Journal of Marriage and Family, Qualitative Health Research, Journal of Contemporary Ethnography, Qualitative Sociology, and Symbolic Interaction. Works Cited: Gimlin, Debra L. (2002). Body Work: Beauty and Self-Image in American Culture. Berkeley, CA: University of California Press. Williams, Christine and Catherine Connell. (2010). “Looking Good and Sounding Right: Aesthetic Labor and Social Inequality in the Retail Industry,” Work and Occupation 37 no. 3: 349-77.  by Dr. Emily Nicholls, Lecturer, University of Portsmouth, UK Professor Victoria Robinson, Director, Centre for Women’s Studies at University of York, UK Dr. Lisa Farndon, Podiatric Development Facilitator, Sheffield Teaching Hospitals, UK 'Stiletto heels, they can put you in another world. It's how you walk and how you carry yourself.’ (Elizabeth, 80s) What is it about shoes? From Dorothy’s red shoes in the Wizard of Oz to Cinderella’s glass slippers, shoes are imbued with meaning and significance, with Pond arguing that shoes ‘seem to have the magic power to make you into someone else’ (1985: 13). Stepping into the right pair can even take you to ‘another world’, in the words of 80-year old Elizabeth, a participant in a recent research project* involving patients and foot health specialists in the UK. For many of us, wearing shoes is both a physical, embodied experience and a way to express our self-image and aspects of our identity (Seferin and Van der Linden, 2012, Branthwaite et al., 2013, Farndon et al., 2016). But for those with complex and long-term health conditions, shoe choice may be more intimately bound up with issues of mobility, health, (dis)ability and the ways in which one’s identity is displayed to others and informed by the diverse relationships we have with one another. Our recent project sought to explore some of the reasons why patients – including those with more complex health needs – may be reluctant to make changes to their shoe choices and may encounter barriers to acting on the advice of podiatrists (Vernon et al., 2011). From bunions and blisters to severe foot pain, deformities and neuropathy, the conditions experienced by those accessing Podiatry Services can have a significant impact on overall health, well-being and mobility, particularly for those with complex health needs who may be at risk of complications, such as amputation. Research shows there is a real correlation between ill-fitting footwear and increased risk of pain, falls, calluses, blisters and ulcers (Parnés, 2007), yet a significant proportion of people with complex health needs wear ill-fitting shoes (Harrison et al., 2007; Silver et al., 2011) and podiatrists and other foot care specialists frequently report difficulties in encouraging patients to make real changes to their footwear. This project brought together a diverse team of researchers previously from the University of Sheffield and expert practitioners from Podiatry Services, Sheffield Teaching Hospitals to explore some of these tensions and consider how they might be resolved in practice. Our work builds directly on a previous UK ESRC funded project, ‘If the Shoe Fits, Footwear, Identification and Transition’ involving one of the research team (Vicki Robinson), which showed the centrality of footwear to individuals' sense of their embodied identity. This more recent project involved interviews with podiatrists, shoe fitters and their patients; with several of the patient participants taking part in follow-up interviews and completing ‘shoe diaries’ to chart their everyday, lived experiences of choosing and wearing shoes. Some of the patients involved in the study had complex, long-term health conditions and were accessing Podiatry Services alongside receiving support from other services as part of managing conditions such as cancer and diabetes. We noted that these participants were often engaged in complex processes of managing their health, well-being and identities, with shoe choice playing a role in this. For these participants, shoes occupied a dual position as both an aid or impediment to mobility and health yet also a key part of dress and appearance, with shoes often playing a role in how identity as ‘sick’ or ‘well’ was portrayed to others and at times acting as ‘a symbol displayed by owners to reinforce their self-image’ (Gillath et al., 2012: 424). Several of the participants with more complex health needs prioritised physical comfort over fashion and described a discrepancy between the types of shoes they would like to wear and the types of shoes that they actually wore, as illustrated by Frank, a diabetic in his 50s:
These findings to an extent challenge the assumption that podiatrists and patients have different – even opposite – priorities and values; moving beyond this dichotomy allows us to recognise that physical comfort and pain reduction may constitute shared priorities that can form a useful starting point for practitioner-patient consultations, particularly for patients with complex needs. However, for those patients who did make considerable changes to their shoe choices, this could be associated with particular costs:
Nigel had at the time of interview been very recently diagnosed with diabetes, and the difficulties he experienced in making various lifestyle changes – such as changing diet - were apparent. In particular, Nigel’s recent adoption of what he called ‘fuddy duddy’ velcro shoes appeared to undermine his sense of himself as a ‘young lad’ and to redefine him as a ‘disabled person’. Shoes were crucially bound up with pride and identity for Nigel, and with his sense of what it means to be a man. The changes he was making to his footwear might be viewed on the one hand as positive steps towards adopting ‘healthier’ footwear, but this came with real consequences including social isolation and withdrawal and a sense that part of his old identity was ‘missing’. This builds on previous research with patients with chronic and long-term health conditions; for example Goodacre and Candy (2011) report that for women with Rheumatoid Arthritis, restricted shoe choice may limit their ability to present themselves to others in the way they desire. Other participants with complex health needs were more resistant towards making changes to their shoe choices, in part because physical comfort was not always their priority. The emotional, psychological and social aspects of ‘comfort’ were also mentioned, echoing Seferin and Van der Linden’s (2012) point that distinctions can be drawn between physical comfort and psychological comfort:
Megan was in her 40s and had experienced a number of health complications, including recently having a stroke. She also suffered from a neuroma – a ‘nerve tumour’ between her toes – and very severe foot pain. Shoes remained an extremely important and central part of Megan’s life, holding an almost transformative power for her in some contexts, where she described stepping into the ‘right’ pair of shoes as giving her bodily confidence and a sense of belonging. Part of her resistance to podiatrist advice around changing her footwear was linked to maintaining a sense of ‘control’ over her body, as she felt this was one of the only areas relating to her health and lifestyle where she could make her own decisions in the face of the numerous other lifestyle changes, medical interventions and treatment programmes required:
Whilst Nigel felt that his revised shoe choices redefined him as ‘disabled’, part of the reason that Megan refused to change her shoes was tied to her resistance to be defined by her condition:
Likewise, Colin who was in his early 50s and was undergoing chemotherapy for cancer identified a tension between accepting the constraints that his ‘condition’ put on him and a need to retain a sense of ‘dignity’:
These examples highlight how shoes occupy a dual and arguably contradictory position as both an aid to mobility (like walking aids and grab rails) yet also a key part of dress and appearance, meaning individuals with complex health conditions may experience tensions and difficulties in their attempts to make shoe choices that provide physical comfort yet also convey their identity in the ‘right’ way to others. It may be that retaining some control over shoe choice through avoiding wearing ‘the grandfather shoes’ allowed participants to feel a sense of dignity and choice in light of the embodied, daily experiences of pain felt in bodies that they themselves defined as a ‘problem’. Such decisions marked a refusal to be defined solely by their medical condition and part of an ongoing process of carrying on ‘as I always have’ despite changes in their health and mobility, as well as an attempt to blend in and minimise the attention drawn to the perceived limitations and ‘problems’ of their own bodies. As Hockey et al. (2013) suggest, footwear can be used as a ‘vehicle’ to provide insights into who we are or – perhaps more importantly - who we want to be; for some of the participants resisting the changes to footwear suggested by podiatrists and continuing to wear the shoes they liked became a tool to resist being read as ‘sick’ or ‘disabled’. These findings suggest that consideration of some of the ways in which patients’ foot conditions and shoe requirements intersect with long-term, chronic and complex health conditions is extremely important. Clearly, recognising the links between people’s shoes and wider sense of who they are is crucial if podiatrists are to help patients to make sustainable changes to their footwear habits that do not simultaneously have a negative impact on their sense of self and well-being. As part of this, an understanding of the ways in which shoes may work towards constructing or resisting particular types of embodied identity is critical. * This collaborative project was funded through the University of Sheffield's Impact, Innovation and Knowledge Exchange (IIKE) scheme, with a contribution of time, resources and expertise from Sheffield Podiatry Services, Sheffield Teaching Hospitals, UK. The findings of the study have been used to develop an online footwear ‘toolkit’ to assist foot health professionals as part of their training and to inform and develop practice. This website and associated tools and publications have been designed to highlight and explore potential barriers to changing footwear and support practitioners to engage in dialogue with patients to address these barriers in ways that take patients’ preferences, motivations and values into consideration. The full footwear toolkit is available at http://www.sheffield.ac.uk/podiatrytoolkit References BRANTHWAITE, H., CHOCKALINGAM, N., GROGAN, S., et al. 2013. Footwear choices made by young women and their potential impact on foot health. Journal of Health Psychology, 18, 1422-1431. FARNDON, L., ROBINSON, V., NICHOLLS, E, and VERNON, W. 2016. If the shoe fits: development of an on-line tool to aid practitioner/patient discussions about ‘healthy footwear’. Journal of Foot and Ankle Research, 9(17), pp. 1-6. GILLATH, O., BAHNS, A. J., GE, F., et al. 2012. Shoes as a source of first impressions. Journal of Research in Personality, 46, 423-430. GOODACRE, L. J. & CANDY, F. J. 2011. ‘If I didn’t have RA I wouldn’t give them house room’: the relationship between RA, footwear and clothing choices. Rheumatology, 50, 513-517. HARRISON, S., COCHRANE, L., ABBOUD, R., et al. 2007. Do patients with diabetes wear shoes of the correct size? Int J Clin Pract, 61, 1900-4. HOCKEY, J., DILLEY, R., ROBINSON, V., et al. 2013. Worn Shoes: Identity, Memory and Footwear. Sociological Research Online, 18, 20. PARNÉS, A. 2007. If the shoe fits…footwear and patients with diabetes. International Journal of Clinical Practice, 61, 1788-1790. POND, M. 1985. Shoes Never Lie, New York, Berkley Publishing Group. SEFERIN, M. & VAN DER LINDEN, J. 2012. Protection or pleasure: female footwear. Work: A Journal of Prevention, Assessment and Rehabilitation, 41, 290-294. SILVESTER, R. N., WILLIAMS, A. E., DALBETH, N., et al. 2011. Choosing shoes: A preliminary study into the challenges facing clinicians in assessing footwear for rheumatoid arthritis patients. Journal of Foot and Ankle Research, 4, O43. VERNON, W., BORTHWICK, A. & WALKER, J. 2011. The management of foot problems in the older person through podiatry services. Reviews in Clinical Gerontology, 21, 331-339.  by Stacey Livingstone
PhD Candidate in Sociology University of California, San Diego “Feminism is the cancer of civilization.” Although online misogyny has been well noted and characterized as par for the course (Gray 2012; Mantilla 2013), it seems surprising to find the above antifeminist statement on what is arguably the most popular online discussion forum for anorexic men due to the fact that anorexic men are in possession of a stigmatized identity (Rich 2006), a trait that theoretically would make them capable of greater empathy than their non-stigmatized counterparts (Zerubavel and Wright 2012). Indeed, it might even be assumed that anorexic men would have greater empathy for feminists especially considering the fact that the oppression the latter are attempting to challenge is based on a gender ideology that has the potential to adversely affect anorexic men (Andersen 1990; Brumberg 2000). Yet this study which subjected an online forum for anorexic men to a discourse analysis discovered that antifeminist sentiment as well as discourses on essentialized difference were quite prevalent: an especially peculiar finding when one reflects on the fact that the central purpose of the forum is to foster a supportive environment for men with an eating disorder. Unsurprisingly, themes also emerged surrounding the body and I argue that the prevalence of discourses on essentialized difference and antifeminist sentiment can be connected to the body projects anorexic men are engaged in. The first theme to emerge was a resounding and widespread desire for the anorexic body coupled with performing this body online: a feat accomplished via discussions concerning everything from exercise regimes and fasting to the repercussions of anorexia. These findings converge with those of recent studies of online pro-ana communities where women exalt an emaciated physique (Fox, Ward and O’Rourke 2005) as well as attempt to make the anorexic body evident online (Boero and Pascoe 2012). In fact, the complete absence of scholarship on men’s engagement in pro-ana communities led me to pursue this study in the first place (Boero and Pascoe 2012; Giles 2006; Haas et al. 2010): a lacuna certainly emanating from the historical association between anorexia and femininity (Brumberg 2000). Although the bodily component of hegemonic masculinity is constantly in flux with its most recent reconceptualization being one of lean muscularity, and although open scrutinizing of the male body is more prevalent now than ever before with the unsurprising result of increased body dissatisfaction and dieting among men (Ricciardelli, Clow and White 2010) – noted conduits to eating disorders (Brumberg 2000) -, I remain unconvinced that the anorexic men on this forum are the victims of excessive conformity to bodily ideals as anorexic women are often portrayed (Fox, Ward and O’Rourke 2005). My interpretation comes from the fact that the men on the forum constantly express desire for a “fragile,” “tiny,” “airy” body: a finding that diverges from Bennett and Gough’s (2012) study of an online forum for dieting men where users constantly framed their dieting as a quest for muscularity. Instead, it appears that the anorexic men of my study were pushing back against hegemonic masculinity as opposed to relentlessly pursuing it. Lending credence to this theory is the fact that many straight-identified users on the forum comment that while they realize their emaciated frames turn off women, they still want fragile bodies: that this body project is being undertaken for them and not in the pursuit of women. This particular finding is important as it not only highlights the counterhegemonic nature of this body project, but further challenges scholars who have suggested that anorexic men tend to be gay on account of their subculture’s exaltation of thinness: a notion that exists within popular culture as well (Herzog, Bradburn and Newman 1990; McVittie, Cavers and Hepworth 2005). Oftentimes the assertion that this body project is being undertaken solely for personal enjoyment revolves about the notion of independent thinking: a discourse that is itself an enactment of hegemonic masculinity (Gill, Henwood and McLean 2005). Yet this notion of independent thinking could in fact be indicative of a pro-ana presence on the forum. As the pro-ana movement combats the notion that anorexia is a mental illness, reframing it as a personal choice and superior lifestyle predicated on control, empowerment and beauty (Fox, Ward, and O’Rourke 2005), it is possible that many users on the forum are engaged in a counterhegemonic project targeting more than just the bodily ideal of masculinity. However, not all of the men on the forum are pro-ana, a finding that is in alignment with recent literature on such sites (Wooldridge, Mok and Chiu 2013), as many have lamented their inability to recover for reasons that will be addressed below. Yet while many users on the forum may be combatting the notion that anorexia is a mental disorder, what is apparent is the fact that many users – straight and gay - are definitely combatting the bodily ideal of hegemonic masculinity. Perhaps this is akin to the feminist approach of viewing anorexia as a form of protest rather than as an instance of over-conformity (Ward 2007). Yet while the feminist perspective of anorexia hinges upon contesting unequal gender relations at the site of the body, the men on the forum I studied do not appear to be fasting away the body associated with gender domination. In fact, many of the members discourse on essentialized difference as reality (as opposed to dominant ideology) and, as mentioned at the start of this blog entry, a very prevalent topic of conversation on the forum is anti-feminism: a trend that cannot be attributed to trolls as I specifically only coded posts written by members of the forum (as opposed to guests) Indeed, many men on the forum bemoan the fact that they are feminized on account of their emaciated bodies: oftentimes through the fag discourse (Pascoe 2012). However, such censuring is never on account of being anorexic, but rather for not meeting the bodily standard of hegemonic masculinity. In fact, many members on the forum lament that their anorexic bodies - as indicative of anorexia - are invisible to family members, peers, school personnel and even medical professionals. As a result, many men on the forum divulge that they cannot get the help that they need: a finding that lends credence to Eliot and Baker’s (2001) supposition that the historical connection between anorexia and femininity continues to be a major obstacle to the proper diagnosis and treatment of anorexic men. Many men on the forum are aware of this connection and are resentful of the double standard it creates with respect to the way their anorexia is treated (i.e. ridiculed or rendered invisible) versus the way the disordered eating habits of their female peers or family members are handled with gravity. In fact, I believe that forum members’ experiences with prejudice in the real world combined with the perceived discrimination they face online – as women frequently post on the forum looking for ana boyfriends or male ana buddies – is one reason why antifeminist sentiment is so prevalent on the site as men’s movements have provided men with the script that the gendered prejudice and discrimination men face today are the results of feminism (Jordan 2016). Another potential reason for the antifeminism on the forum may be the fact that subordinate men, although they may contest the internal dimension of hegemonic masculinity that negatively affects them, tend to uphold the external dimension as it continues to exalt them in the face of debasement (Oliffe 2006; Yeung, Stombler and Wharton 2006). From this lens, the desire for thinness circulating throughout the forum indicates an attempt to undermine the internal dimension of hegemonic masculinity alone by rejecting the physical component of the ideal as opposed to an attempt to undermine the entirety of the gender order. This hypothesized strategy is perhaps made more evident by the partial penetration of gender ideology undertaken by forum members - a penetration that highlights the ways in which men suffer at the hands of gendered beliefs while leaving essentialized difference intact – as well as the targeting of feminists who would dismantle the entirety of the gender order that benefits even subordinate men. Surprisingly, many of the forum members engaging in such partial penetrations are transmen. Additionally, like their cisgender counterparts, they too desire thinness; only their desire revolves about starving away the curves of femininity. Like the body projects of their cisgendered counterparts, the body projects undertaken by the transmen on this forum do not dovetail with the feminist notion of anorexia as protest as transmen on the forum additionally uphold notions of essentialized difference and engage in antifeminist discourse. Another surprising finding is the fact that transmen are resoundingly accepted on the forum: not merely tolerated, but actually accepted as men. This is an interesting finding given how widespread transphobia tends to be in general (Girshick 2008), how men tend to be more transphobic than women (Nagoshi, et al. 2008) and how prevalent discourses on essentialized difference are on the forum: a discourse that conflates sex and gender. Perhaps such trans-acceptance from cisgendered members stems from the fact that their experiences with subordinate masculinity have made them more empathetic towards other subordinate masculinities. Or perhaps it stems from the fact that this community of anorexic men exists online. While the offline bodies of transmen might make cisgendered anorexic men feel uncomfortable, online, trans-identified users are not only perhaps able to more successfully perform gender identity through discourses on essentialized difference and anti-feminist sentiment - as their material bodies that might produce cognitive dissonance in cisgendered members are hidden-, they are also able to perform a masculine bodily identity through discourses that make their anorexic body (which, in this context, is their masculine body) evident online (Boero and Pascoe 2012). In light of this hypothesis, the simultaneous presence of trans-acceptance and talk of essentialized difference may now make sense. As many transmen, like their cisgendered counterparts, discourse on essentialized difference, they contribute to the presence of this conversation on the forum: a contribution that not only intensifies this discursive trend, but also perhaps paves the way for their acceptance as real men within this online context. While such gender presentation may only be strategic, there is also the possibility that it is heartfelt especially when one considers the fact that certain feminists have and continue to be transphobic. Certainly, this initial study opens the door for further investigations. One thing that I must do personally in the future is tease out any distinct subgroups on the forum, as it is most likely that a few exist and would perhaps account for the seeming incongruity of some of my findings. References: Andersen, Andrew. 1990. “Diagnosis and treatment of males with eating disorders.” Pp. 133-162 in Males with Eating Disorders edited by Andrew Andersen. New York: Brunner/Mazel. Bennett, Eleanor and Brendan Gough. 2012. “In Pursuit of Leanness: The Management of Appearance, Affect and Masculinities within a Men’s Weight Loss Forum.” Health 17(3):284-299. Boero, Natalie and C.J. Pascoe. 2012. “Pro-anorexia Communities and Online Interaction: Bringing the Pro-ana Body Online.” Body & Society 18(2):27-57. Brumberg, Joan Jacobs. 2000. Fasting Girls: The History of Anorexia Nervosa. New York: Vintage Books. Eliot, Alexandra O. and Christina Wood Baker. 2001. “Eating Disordered Adolescent Males.” Adolescence 36(143):535. Fox, Nick, Katie Ward and Alan O’Rourke. 2005. “Pro-anorexia, weight-loss drugs and the internet: an ‘anti-recovery’ explanatory model of anorexia.” Sociology of Health & Illness 141:944-971. Giles, David. 2006. “Constructing identities in cyberspace: The case of eating disorders.” British Journal of Social Psychology 45:463-477. Gill, Rosalind, Karen Henwood and Carl McLean. 2005. “Body Projects and the Regulation of Normative Masculinity.” Body and Society 11(1):37-62. Girschick, Lori B. 2008. Transgender Voices: Beyond Women and Men. Lebanon, NH: University Press of New England. Gray, Kishonna L. 2012. “Intersecting Oppressions and Online Communities.” Information, Communication and Society 15(3):411-428. Haas, Stephen M., Meghan E. Irr, Nancy A. Jennings and Lisa M. Wagner. 2010. “Communicating thin: A grounded model of Online Negative Enabling Support Groups in the pro-anorexia movement.” New Media & Society 13(1):40-57. Herzog, David B., Isabel S. Bradburn, and Kerry Newman. 1990. “Sexuality in Males with Eating Disorders.” Pp. 40-53 in Males with Eating Disorders edited by Arnold E. Andersen. New York: Brunner/Mazel. Jordan, Ana. 2016. “Conceptualizing Backlash: (UK) Men’s Rights Groups, Anti-feminism and Postfeminism.” Canadian Journal of Women and the Law. Coming Soon. Mantilla, Karla. 2013. “Gendertrolling: Misogyny Adapts to New Media.” Feminist Studies 39(2):563-570. McVittie, Chris, Debbie Cavers and Julie Hepworth. 2005. “Femininity, Mental Weakness, and Difference: Male Students Account for Anorexia Nervosa in Men.” Sex Roles 53(5/6):413-418. Nagoshi, Julie L., Katherine A. Adams, Heather K. Terrell, Eric D. Hill, Stephanie Brzuzy and Craig T. Nagoshi. 2008. “Gender Differences in Correlates of Homophobia and Transphobia.” Sex Roles 59(7-8):521-531. Oliffe, John. 2006. “Embodied Masculinity and Androgen Deprivation Therapy.” Sociology of Health and Illness 28(4):410-432. Pascoe, C.J. 2012. Dude You’re a Fag: Masculinity and Sexuality in High School. Berkeley: University of California Press. Ricciardelli, Rosemary, Kimberley A. Clow and Philip White. 2010. “Investigating Hegemonic Masculinity: Portrayals of Masculinity in Men’s Lifestyle Magazines.” Sex Roles 63:64-78. Rich, Emma. 2006. “Anorexic dis(connection): managing anorexia as an illness and an identity.” Sociology of Health and Illness 28(3):284-305. Ward, Katie J. 2005. “I Love You to the Bones: Constructing the Anorexic Body in Pro-Ana Message Boards.” Sociological Research Online 12(2). Wooldridge, Tom, Caroline Mok and Sabrina Chiu. 2013. “Content Analysis of Male Participation in Pro-Eating Disorder Web Sites.” Eating Disorders: The Journal of Treatment and Prevention 22(2):97-110. Yeung, King-To, Mindy Stombler and Renee Wharton. 2006. “Making Men in Gay Fraternities: Resisting and Reproducing Multiple Dimensions of Hegemonic Masculinity.” Gender and Society 20(1):5-31. Zerubavel, Noga and Margaret O’Dougherty Wright. 2012. “The dilemma of the wounded healer.” Psychotherapy 49(4):482-491. |
Discuss!Guest bloggers discuss hot topics, teaching ideas, and research dilemmas on bodies. Archives
August 2020
Categories |



 RSS Feed
RSS Feed
